
REFLUX · 6-MIN READ · UPDATED MAY 2026
Why Gastric Sleeve Can Cause Acid Reflux
Up to 1 in 3 sleeve patients develop new or worsened acid reflux after surgery. Here’s the anatomical reason — and what predicts who will be affected.
By Dr. Alejandro López · Medically reviewed · Posted in Blog
See if you qualify in 2 minutes
Answer a few questions about your health and weight loss goals — our bariatric team reviews your answers and recommends the right procedure for you. No cost, no commitment.
Start my evaluation →TL;DR
Gastric sleeve removes the part of the stomach that produces gastrin, but the high-pressure tube anatomy + lower esophageal sphincter changes can cause acid reflux in 20-30% of patients. Untreated, it can progress to esophagitis or Barrett’s esophagus. The most effective surgical solution is conversion to Roux-en-Y gastric bypass.
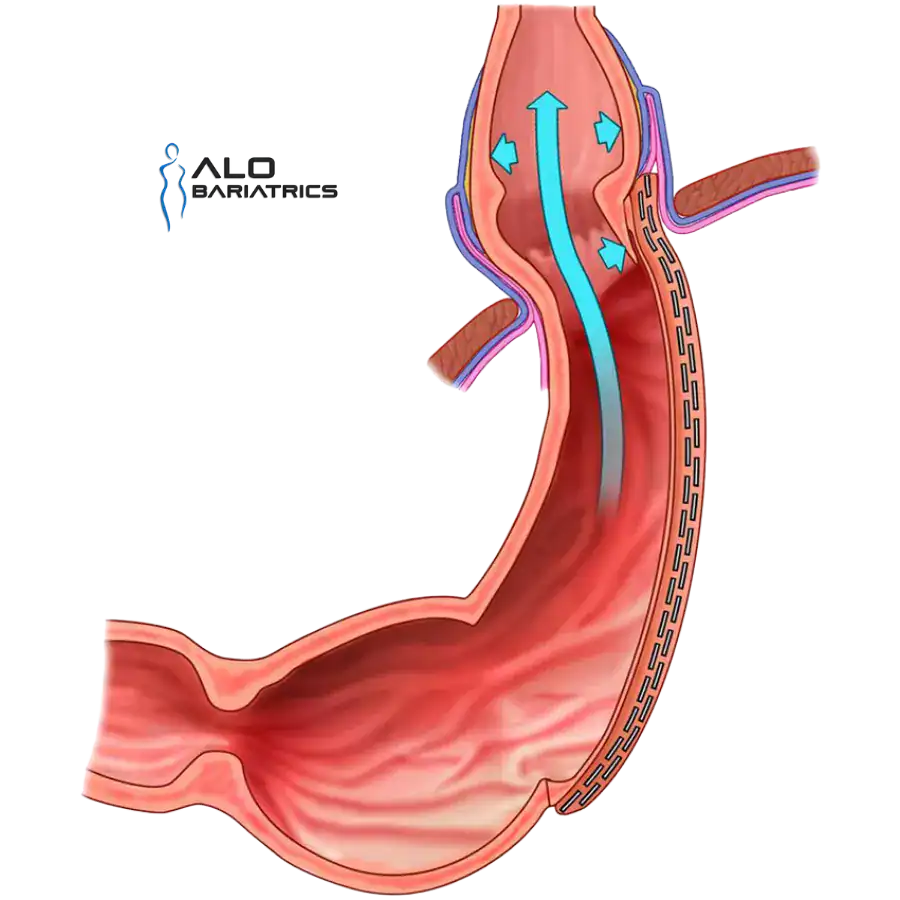
How the Sleeve Procedure Changes Reflux Anatomy
The gastric sleeve removes about 80% of the stomach, leaving a narrow tube. While this restricts food intake and reduces hunger hormones, it also fundamentally changes the anatomy that prevents reflux:
- Increased intragastric pressure — the tube-shaped stomach has higher internal pressure than the J-shape
- Disrupted angle of His — the natural sharp angle between the esophagus and stomach is lost
- Weakened lower esophageal sphincter — fundus removal affects the sphincter muscle support
- Hiatal hernia exposure — small undiagnosed hiatal hernias become symptomatic
These four mechanisms combined explain why even patients with NO reflux before surgery may develop it after.
Who Is at Highest Risk?
Not every sleeve patient develops reflux. Studies consistently identify these risk factors:
- Pre-existing GERD — patients with mild reflux before surgery often see it worsen
- Undetected hiatal hernia — present in up to 40% of obese patients
- BMI > 50 — higher abdominal pressure increases risk
- Female sex — slight increased risk in women
- Smoking history — affects sphincter function
This is why an experienced bariatric team performs routine hiatal hernia screening before surgery and offers concurrent hernia repair when needed.
What to Do If You Have Reflux After Sleeve
Treatment depends on severity and how long the reflux has persisted:
- Mild reflux: Proton pump inhibitors (PPIs) + diet modifications + weight loss work for ~60% of cases
- Moderate-persistent reflux: Endoscopy to evaluate esophagitis, plus continued medical management
- Severe / Barrett’s esophagus: Surgical revision — most commonly sleeve-to-bypass conversion
- Hiatal hernia recurrence: Focused repair, possibly without revision
The good news: surgical revision resolves reflux in 90%+ of patients when sleeve anatomy is the cause.
If you're considering gastric sleeve but already have moderate-to-severe reflux, gastric bypass may be the better option for you — it actually fixes reflux instead of worsening it. ALO Bariatrics offers both gastric bypass and sleeve-to-bypass revision for patients who develop reflux after their sleeve.
When to See a Bariatric Surgeon
You should consult a surgeon if you experience:
- Reflux symptoms more than 2x/week despite PPIs
- Difficulty swallowing or food sticking
- Persistent cough or hoarseness
- Esophagitis or Barrett’s diagnosis on endoscopy
- Weight regain combined with reflux
Dr. Alejandro López has performed over 2,000 bariatric procedures including sleeve revision surgeries. Free initial evaluation available.
Frequently Asked Questions
Is reflux after gastric sleeve normal?
Can I take medication forever instead of getting revision?
How effective is sleeve-to-bypass conversion for reflux?
Will I lose weight after sleeve-to-bypass conversion?
Have Reflux After Your Gastric Sleeve?
Get a free evaluation with Dr. Alejandro López. We’ll review your case and recommend the right surgical solution.
Request Free Evaluation →