
COMPARISON · 8-MIN READ · UPDATED APR 2026
Gastric Bypass vs Gastric Sleeve: What's the Difference and Which Is Right for You?
Both produce dramatic weight loss. Both reverse diabetes. But they work differently — and one is clearly better for certain patients. Here is the honest side-by-side comparison.
By Dr. Alejandro López, MD · Bariatric Surgeon · Tijuana · Guadalajara · Puerto Vallarta
The Short Version
- Sleeve: simpler surgery, faster recovery, 60–70% excess weight loss, lower complication rate.
- Bypass: more complex, 70–80% excess weight loss, better for diabetes and reflux.
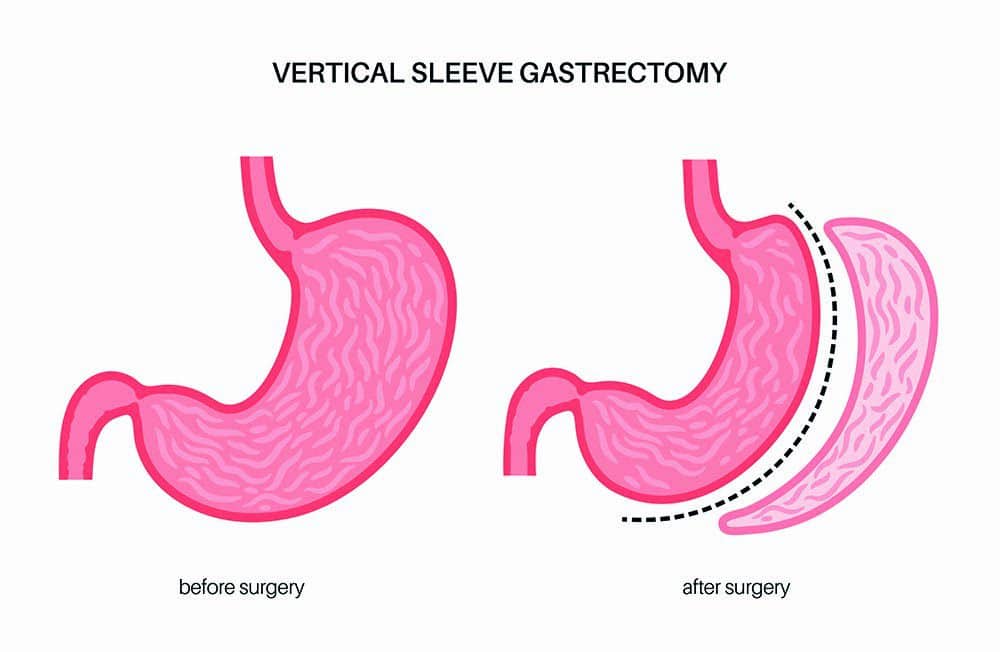
- Sleeve: removes 80% of stomach but does NOT alter intestines.
- Bypass: creates small pouch + reroutes intestine — restrictive AND malabsorptive.
- The right choice depends on YOUR BMI, diabetes status, GERD, and goals.
Gastric bypass and gastric sleeve are the two most common bariatric procedures in the world — accounting for over 90% of all bariatric surgeries. Both work, both have decades of data, both transform lives. But they are different procedures with different trade-offs.
This guide compares gastric bypass with gastric sleeve (manga gástrica) head-to-head — when each is the better choice, the trade-offs of each, and how to decide.
How They Differ Anatomically
Gastric sleeve removes 80% of the stomach, creating a banana-shaped sleeve. The intestines are not touched. The result: smaller stomach holds less food, hormonal changes from removing the fundus reduce hunger. Purely restrictive procedure.
Gastric bypass creates a small stomach pouch (30 ml) and reroutes food past the upper intestine, reconnecting further down. Restrictive (small pouch) AND malabsorptive (skipped intestine). The rerouting creates strong hormonal changes that explain the superior diabetes reversal rates.
6 Differences Between Bypass and Sleeve
DIFFERENCE 1 OF 6
Weight loss — bypass wins by 10%
Bypass: 70–80% excess weight loss at 1 year, sustained at 5 years. Sleeve: 60–70%. For a patient with 50 kg excess weight, that is 5 kg difference. Marginal for most patients; significant for some.
DIFFERENCE 2 OF 6
Diabetes — bypass is the clear winner
Bypass produces complete remission of type 2 diabetes in 60–80% of patients. Sleeve: 40–60%. The hormonal changes from rerouting food are more powerful than from sleeve alone. For diabetes severe with multiple medications, bypass is the better tool.
DIFFERENCE 3 OF 6
GERD/Reflux — bypass cures, sleeve can cause it
Bypass resolves pre-existing GERD in 80%+ of patients. Sleeve CAN CAUSE OR WORSEN GERD in 10–30% of patients. If you have significant pre-op reflux or hiatal hernia, bypass is the safer choice. Sleeve is for patients without significant reflux.
DIFFERENCE 4 OF 6
Complication rate — sleeve has the edge
Sleeve major complication rate: 2–3%. Bypass: 3–5%. Slightly higher with bypass because of intestinal anastomoses. Both are very safe in experienced hands.
DIFFERENCE 5 OF 6
Recovery and lifestyle — sleeve is simpler
Both: 1–2 nights hospital, 6 weeks to full activity. Sleeve patients have less restriction on what foods to avoid. Bypass patients need to avoid sugar-heavy foods due to dumping syndrome risk. Sleeve patients usually report easier “lifestyle” recovery.
DIFFERENCE 6 OF 6
Reversibility — neither truly reversible
Sleeve removes stomach permanently — cannot be undone (the removed 80% is gone). Bypass technically CAN be reversed but it is complex revisional surgery rarely performed. Treat both as permanent decisions.
📌 Bypass vs Sleeve — The Decision Framework
For most patients without severe GERD or diabetes, sleeve is the simpler and safer first choice. For patients with severe diabetes (especially long-standing) or significant reflux, bypass is the better tool. Neither is universally “better” — both are excellent procedures for the right patient. The decision should be made with an experienced cirujano bariatra who evaluates YOUR specific case.
When to Choose Each
Choose sleeve when: BMI 35–50, no severe GERD, no diabetes or mild diabetes, want simpler surgery and easier recovery.
Choose bypass when: BMI 35–50 with type 2 diabetes (especially long-standing), severe GERD or hiatal hernia, want best diabetes reversal data.
Consider neither (yet) when: BMI 30–35 without comorbidities — start with balón gástrico or GLP-1 medications.
Consider switch duodenal when: BMI 50+ or severe long-standing diabetes — sleeve or bypass may be insufficient.
Common Mistakes Choosing Between Sleeve and Bypass
Choosing sleeve because “it is simpler” when you have severe diabetes. Bypass is the more effective tool for diabetes. Skipping it to save 30 minutes of operating time costs you 20% lower remission rate.
Choosing bypass for severe GERD without trying conservative measures first. If reflux is mild, sleeve + PPI may work. Bypass is reserved for moderate-severe cases.
Choosing the procedure your friend had. Your friend’s case is not yours. BMI, comorbidities, age, surgical history all matter.
Picking based on cost difference. $1,000 difference between sleeve and bypass is negligible compared to 10 years of life impact.
Not considering long-term outcome data. Bypass has 50+ years of data; sleeve has 20+. Both are robust but bypass has longer track record.
Letting fear of intestinal rerouting drive sleeve decision. Bypass reroutes the intestine but the connection works the same as your normal anatomy. Not a “more dangerous” procedure.
Sleeve or bypass for YOUR case?
Free 15-min consultation. We evaluate your BMI, diabetes status, GERD history, and goals — and recommend the procedure that fits YOUR case best. No bias toward one or the other.
Frequently Asked Questions
Which loses more weight: bypass or sleeve?
Bypass produces 70–80% excess weight loss; sleeve 60–70%. For most patients the difference is about 5 kg over a year. Bypass has slight edge but sleeve is also highly effective.
Which is better for diabetes?
Bypass is the clear winner — 60–80% complete remission of type 2 diabetes vs 40–60% with sleeve. For patients with significant diabetes, bypass is the more effective tool.
Which is safer?
Sleeve has slightly lower complication rate (2–3% vs 3–5% for bypass) because it does not involve intestinal anastomoses. Both are very safe in experienced hands.
Can I convert from sleeve to bypass later?
Yes. Sleeve-to-bypass conversion is well-established revisional surgery, typically performed when persistent GERD or inadequate weight loss. Adds complexity but feasible.
Which has better long-term data?
Bypass has 50+ years of long-term outcome data. Sleeve has 20+ years. Both have proven track records. Bypass slightly more “established” but sleeve has become the most common bariatric procedure worldwide.
How much do each cost in Mexico?
At ALO Bariatrics: sleeve from $4,500 USD all-inclusive, bypass from $5,900 USD. Includes surgeon, hospital, anesthesia, recovery hotel, ground transport.
Will I need vitamins for life with both?
Yes — lifelong supplementation is required after both procedures. Sleeve patients have slightly less malabsorption (only the stomach is altered). Bypass patients need more attention to B12 and iron supplementation due to intestinal rerouting.
One last thing
The “best” between sleeve and bypass depends entirely on YOUR case — your BMI, your diabetes status, your reflux history, your goals. An honest cirujano bariatra evaluates these factors and recommends the right procedure for YOU. If your surgeon has a strong default preference for one over the other in all cases, get a second opinion. The right choice should be specific to your medical case.