
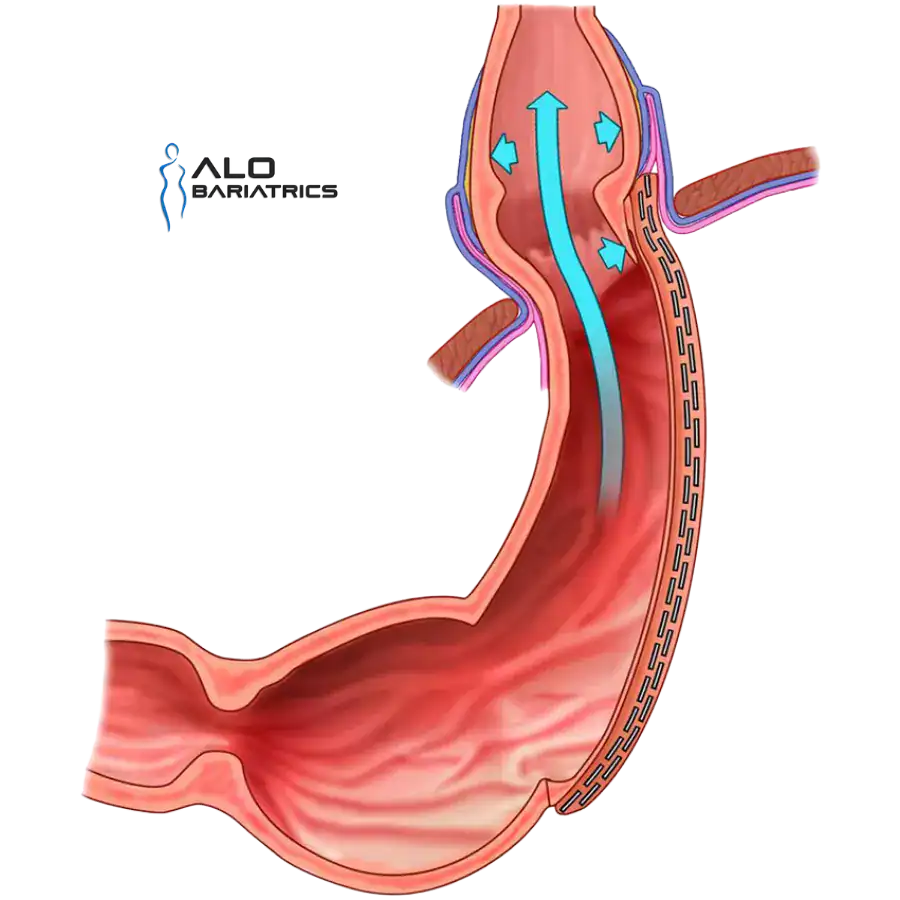
Up to 1 in 3 sleeve patients develop new or worsened acid reflux after surgery. Mild cases respond to proton pump inhibitors, weight loss, and diet changes. But when reflux persists despite medical therapy — or when endoscopy shows esophagitis or Barrett's esophagus — the underlying anatomical problem will not resolve on its own.
Converting a gastric sleeve to a Roux-en-Y gastric bypass eliminates the high-pressure tube anatomy of the sleeve and reroutes acid away from the esophagus. For most patients with severe post-sleeve GERD, this is the most effective long-term solution.
- Persistent GERD symptoms despite maximum-dose PPIs for at least 6 months
- Endoscopic evidence of esophagitis, ulceration, or Barrett's esophagus
- Recurrent or untreated hiatal hernia
- Weight regain combined with reflux relapse
- Fit for laparoscopic surgery confirmed by preoperative evaluation


Dr. Alejandro López, MD, FACS
Bariatric Revision Specialist
- Fellow of the American College of Surgeons (FACS)
- 20,000+ bariatric procedures performed
- Specialized in sleeve-to-bypass conversion and antireflux surgery
- Member of ASMBS, IFSO, and CMCOEM
- Premium hospitals in Tijuana, Guadalajara, and Puerto Vallarta