
SAFETY · 7-MIN READ · UPDATED APR 2026
What Is the Safest Form of Weight Loss Surgery? The Honest Comparison
Manga gástrica has the lowest complication rate among major bariatric procedures. But “safest” depends on YOUR specific medical profile — what is safest for one patient may be wrong for another.
By Dr. Alejandro López, MD · Bariatric Surgeon · Tijuana · Guadalajara · Puerto Vallarta
The Short Version
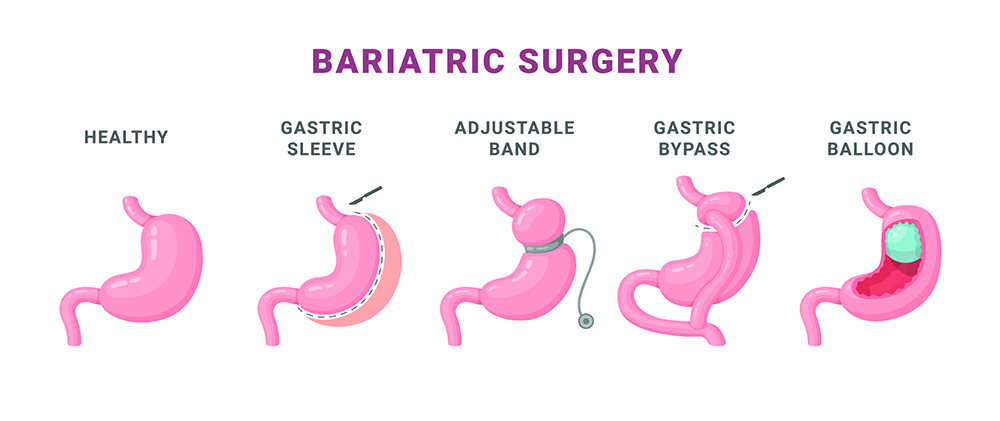
- Manga gástrica: lowest complication rate (2–3%), simplest, no intestinal rerouting.
- Balón gástrico: technically safest (no cirugía) but limited effectiveness.
- Bypass: 3–5% complication rate, slightly more complex but proven over 50 years.
- Switch duodenal: 5–8%, the most complex, reserved for severe cases.
- Surgeon experience matters more than procedure for safety.
“What is the safest weight loss surgery?” is one of the most common questions — and the answer depends on what you mean by “safe” and what your specific case looks like. The procedure with the lowest complication rate (sleeve gastrectomy) is not always the safest for YOU.
This guide compares safety profiles of all major bariatric procedures — manga gástrica, bypass, switch duodenal, balón gástrico — with the honest data so you can decide what is safest for your case.
How "Safety" Is Measured
Safety has multiple dimensions: short-term mortality (30-day), major complication rate, minor complication rate, long-term complications, nutritional risks. A procedure with low short-term mortality may have higher long-term nutrient deficiency risk. “Safest” is multidimensional.
Equally important: SURGEON safety matters more than procedure safety. A “complex” procedure in expert hands is safer than a “simple” procedure in inexperienced hands. Cirujano with 500+ cases per year has 3x lower complication rates than one with 50 cases per year, regardless of which procedure.
6 Procedures Ranked by Safety Profile
RANK 1 OF 6
#1 Balón gástrico — technically safest (no surgery)
Balón gástrico is endoscopic — no incisions, no general anesthesia (only sedation). Major complication rate: under 1%. The trade-off: only 10–15% weight loss, requires removal at 6 months. For BMI 27–35 without diabetes, ideal first option.
RANK 2 OF 6
#2 Manga gástrica — safest major bariatric surgery
Manga gástrica has the lowest complication rate among major bariatric procedures: 2–3% major complications, mortality under 0.3%. Simpler than bypass (no intestinal rerouting), shorter operating time, less recovery. Excellent for IMC 35–50 without severe GERD.
RANK 3 OF 6
#3 Gastric bypass — proven safety over 50 years
Bypass has 3–5% complication rate — slightly higher than sleeve due to intestinal anastomoses. But it has 50+ years of long-term data, the most studied procedure. For diabetes severe and GERD, often the safer LONG-TERM choice despite slightly higher short-term risk.
RANK 4 OF 6
#4 SILS — same safety as sleeve, better cosmetic
SILS (single-incision laparoscopic surgery) performs the same procedures with one incision instead of 4–5. Same safety profile as standard laparoscopic. Requires specialized surgical training. Better cosmetic outcome (cicatriz oculta en ombligo).
RANK 5 OF 6
#5 Mini bypass — safety comparable to standard bypass
Mini bypass has slightly lower complication rate than standard bypass (one anastomosis vs two), but slight risk of bile reflux. For patients without severe pre-op GERD, equivalent or slightly safer than standard bypass.
RANK 6 OF 6
#6 Switch duodenal / SADI-S — most complex, reserved for severe cases
Switch and SADI-S have 5–8% complication rate — the highest among bariatric procedures. But for BMI 50+ or severe diabetes, they produce best weight loss. The “higher” risk is mostly relative — still under 10%.
📌 The Real Safety Framework
“Safest” depends on three factors: the procedure, your medical case, and your surgeon’s experience. Choosing the lowest-complication procedure (sleeve) is wise only if sleeve is right for YOUR case. Choosing an experienced cirujano with high case volume matters more than choosing “the safest procedure” with an inexperienced surgeon. Both factors deserve equal attention.
Choosing the Safest Procedure for YOUR Case
If your BMI is 27–35 and you have no diabetes: Balón gástrico is the safest first step. Manga is the most-safe major surgery.
If your BMI is 35–50 without severe GERD/diabetes: Manga gástrica is the safest choice. Bypass is also safe and may be preferred for diabetes.
If your BMI is 35–50 with severe GERD or hiatal hernia: Bypass is the SAFER choice despite higher complication rate (sleeve makes reflux worse).
If your BMI is 50+ or severe long-standing diabetes: Switch duodenal or SADI-S — more “risky” but the only procedure powerful enough to address your case. Risk is acceptable for the benefit.
In all cases: Choose the most experienced cirujano bariatra you can. Surgeon experience matters more than procedure.
Common Safety Mistakes
Picking sleeve because “it is the safest” when you have severe GERD. Wrong call. Bypass is safer for YOUR case.
Picking the cheapest surgeon. Low-volume surgeons have higher complication rates regardless of procedure.
Choosing switch duodenal for “more weight loss” without needing it. If sleeve or bypass would work, the extra complexity of switch is not worth the higher risk.
Ignoring pre-op evaluation results. Endoscopy findings, cardiac evaluation — all change risk profile. Take them seriously.
Not asking surgeon complication rates. Reputable surgeons share their data. Hesitation to share is a warning sign.
Treating bariatric as “elective” and skipping prep. Pre-op diet, smoking cessation, walking — all reduce surgical risk. Skipping pre-op work increases risk significantly.
Which is safest for YOUR case?
Free 15-min consultation. We evaluate your medical history, comorbidities, BMI and surgical history — and recommend the safest procedure for YOUR specific case. No bias, no pressure.
Frequently Asked Questions
Which bariatric surgery has the lowest complication rate?
Sleeve gastrectomy (manga gástrica) has the lowest complication rate among major bariatric procedures: 2–3% major complications. Balón gástrico is technically safer (under 1%) but not a true “surgery” — endoscopic placement of a device.
Is sleeve safer than bypass?
For most patients, sleeve has slightly lower short-term complication rate (2–3% vs 3–5% for bypass). But “safer” depends on case. For severe GERD or hiatal hernia, bypass is the safer choice long-term despite slightly higher short-term risk.
How dangerous is bariatric surgery overall?
Modern bariatric surgery has mortality under 0.5% — comparable to gallbladder removal. Major complications 2–8% depending on procedure. Risks are much lower than continuing with severe obesity over decades.
Does the surgeon's experience matter more than the procedure?
Yes, significantly. A high-volume surgeon (200+ bariatric cases/year) has 3x lower complication rates than a low-volume surgeon, regardless of procedure. Surgeon experience matters more than procedure choice for safety.
Is bariatric surgery in Mexico as safe as in the US/Canada?
At accredited centres with experienced surgeons, yes — safety outcomes are equivalent. Verify CSG or JCI accreditation, surgeon case volume (200+ per year), and complication rates before choosing.
What is the safest option for BMI 50+?
For severe obesity (BMI 50+), switch duodenal or SADI-S produces the best long-term outcomes despite slightly higher short-term complication rate. The most powerful tool is the right choice for the most severe case.
Can I avoid surgery and just use Ozempic?
For BMI 30–35 without severe diabetes, yes — Ozempic is a reasonable first option. For BMI 35+ with significant comorbidities, the cumulative risk of staying obese (cardiovascular events, diabetes complications) typically exceeds the surgical risk by a wide margin.
One last thing
“What is the safest weight loss surgery?” has no universal answer — it depends on your case and your surgeon. For most patients with moderate obesity and no complications, manga gástrica with an experienced cirujano bariatra is the lowest-risk path. For complex cases, the “safest” procedure may be the most powerful one done by the right team. Discuss your specific situation honestly with a cirujano bariatra who has data to share.